Penn AQM Customer Service Workshop Evaluation
A Penn Medicine case study of a customer-service workshop evaluated with Automated Quality Monitoring, matched comparison agents, and a quasi-difference-in-differences design.
Operating context
Penn Medicine, University of Pennsylvania Health System Patient Engagement Center
October 2025–April 2026
- Role relationship
- Analyst and researcher
- Contribution
- I was the analyst and researcher responsible for the analysis and research/poster work. William R. Stewart, Manager of Quality, and Kristi M. Madden, Manager of Training, are full coauthors whose substantial contributions shaped the design, training, messaging, and leadership communication; Penn Medicine owns the public historical poster.
- Result
- The matched quasi-difference-in-differences evaluation estimated higher Courtesy Phrases and Positive Language after the workshop, with a nonsignificant Average Call Duration balancing result whose interval still permits a possible increase.
The question was whether training changed an observable habit
In a live access center, leadership has to hold two ideas at once: a call should move efficiently, and the patient should hear clear acknowledgement while it does. Penn Medicine's Patient Engagement Center had Automated Quality Monitoring (AQM) measures that made a customer-service opportunity visible, so the operating question asked whether a workshop changed the measured language beyond showing that people attended it.
The project and evaluation ran from October 2025 through April 2026. It became Evaluating a Customer Service Workshop: A Difference-in-Differences Analysis of Contact Center Agent Performance, presented during Patient Access Collaborative (PAC) Annual Symposium poster programming in Columbus on May 14, 2026.
From a measured opportunity to a fair comparison
Training and operations partners selected Courtesy Phrases and Positive Language as the primary AQM behaviors. The workshop used examples, practice, and reinforcement around the small words that make acknowledgement audible in a call: “Can I please have your name and date of birth?” and “Thank you” after a patient answers. This is a representative acknowledgement scene, not a quoted transcript.
The evaluation included workshop attendees with sufficient pre/post Verint AQM observations and contemporaneous comparison agents with usable data matched on available baseline and operating context. The poster gives no numeric observation threshold. The design was a matched, quasi-experimental difference-in-differences (DiD) estimate: it compares change across the same period; it is not randomized evidence and does not prove that training alone caused every observed change.
Evidence folio
The symposium poster
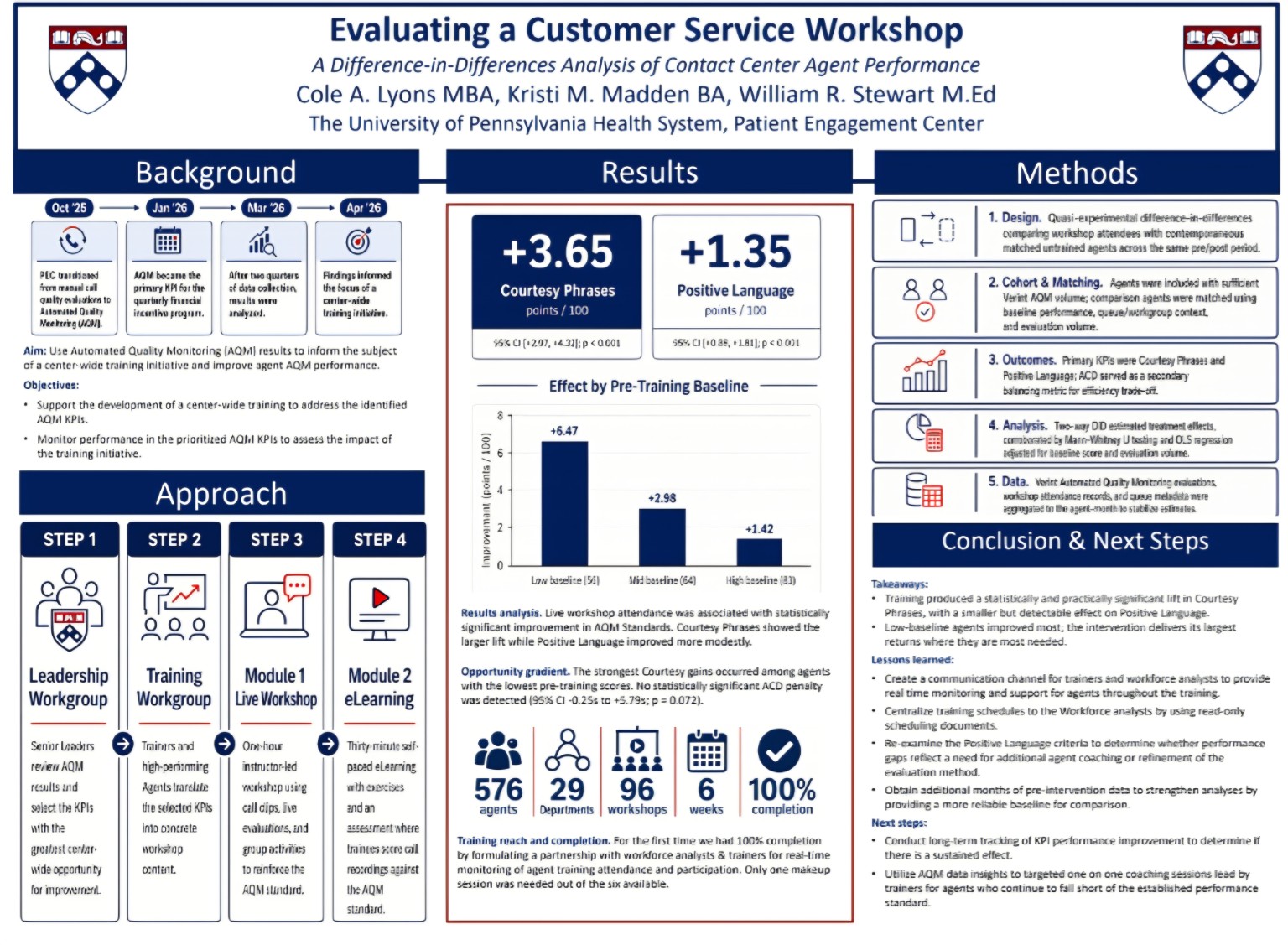
The Penn Medicine poster describes the workshop, matched quasi-difference-in-differences design, language estimates, balancing result, and limitations. A text transcript accompanies the original raster PDF.
Cole A. Lyons, Kristi M. Madden, and William R. Stewart presented the poster during Patient Access Collaborative Annual Symposium programming in Columbus on May 14, 2026.
Download the historical raster poster (PDF, 0.4 MB).
The second group photograph shows the wider Penn team at the symposium in Columbus.

What the estimates say
The two primary language measures moved upward relative to the matched comparison agents. The estimates below are reported exactly in points per 100, with their confidence intervals and p-values.
Difference-in-differences estimates
Measured service language changed after the workshop
Data table
| Measure | Reported estimate | 95% CI | p-value |
|---|---|---|---|
| Courtesy phrases | +3.65 | +2.97 to +4.33 | < 0.001 |
| Positive language | +1.35 | +0.88 to +1.81 | < 0.001 |
| Average call duration | not significant | −0.25 to +5.79 | 0.072 |
Courtesy Phrases rose +3.65 points per 100 (95% CI +2.97 to +4.33, p < 0.001). Positive Language rose +1.35 points per 100 (95% CI +0.88 to +1.81, p < 0.001). These are workshop-associated estimates from a quasi-DiD comparison, not randomized proof.
Average Call Duration (ACD) was the balancing metric, with a 95% CI of −0.25 to +5.79 seconds and p = 0.072; the poster does not provide an ACD point estimate. Because the interval crosses zero, this nonsignificant result leaves the time cost unresolved and cannot support a zero-cost claim.
The opportunity gradient is a coaching signal
Courtesy Phrases showed a descending baseline gradient: +6.47 points per 100 for low-baseline agents, +2.98 for mid-baseline agents, and +1.42 for high-baseline agents.
Opportunity gradient
The lift was largest where the baseline was lowest
Data table
| Baseline tercile | Courtesy-phrase gain |
|---|---|
| Low baseline | +6.47 |
| Mid baseline | +2.98 |
| High baseline | +1.42 |
The gradient helps a training team decide where coaching may be most useful. It should not be read as a precisely larger causal effect for one group: regression to the mean may contribute, even with a contemporaneous matched comparison.
Scale, completion, and credit
The poster reports 576 agents across 29 departments, 96 workshops, and six weeks of delivery. The 100% completion figure refers only to the included training cohort; it is not participation by every agent, every invitation, or the entire Patient Engagement Center.
Cole A. Lyons was the analyst and researcher responsible for the analysis and research/poster work, while William R. Stewart, Manager of Quality, and Kristi M. Madden, Manager of Training, are full coauthors whose substantial contributions shaped the overall design, training, messaging, and leadership communication. Training and operations partners created and delivered the workshop and enabled the evaluation, and Penn Medicine owns the public historical poster.
The boundary of the evidence
Under a matched, quasi-DiD design, the workshop was associated with higher measured Courtesy Phrases and Positive Language. Those language indicators support a connection between observable behavior and fair training, coaching, and operational learning, with the denominator, comparison, and uncertainty kept in view; they leave patient trust, satisfaction, adherence, clinical outcomes, and any general effect of automated monitoring unmeasured.
Notes
The AHRQ CAHPS measures PDF and AHRQ patient-experience overview describe helpful, courteous, and respectful staff as dimensions of patient experience. This evaluation measured language, not patient-reported experience.
Hewitt and colleagues' 2009 naturalistic study, Front desk talk, distinguishes task-centred interaction from polite language and rapport. It is context for the acknowledgement scene, not evidence that these phrases alone cause trust or satisfaction.
The 2024 JAMA research synthesis on word choice supports a broader role for wording in empathy, competence, trust, and encounter outcomes without isolating “please” or “thank you” as sufficient causes.
The official 2026 PAC symposium agenda records the May 14 poster programming. O'Neill and colleagues' controlled pre/post methods comparison explains the assumptions and comparison choices required for difference-in-differences.